
Computer Adaptive Modes
 John McManigle | 15 May 2020
John McManigle | 15 May 2020
This is the sixth video in our Pulmonary and Ventilator Mechanics Chalk Talk Series, where our goals are to learn how a ventilator works, and how to work a ventilator. In this talk, we explore a few examples of the endless possibilities opened up by computer-controlled ventilator valves and sensors. Specifically, we look at volume support, proportional assist ventilation, automatic tube compensation, and mandatory minute ventilation. One important thing to remember in these more "advanced" ventilator modes is that they differ from ventilator to ventilator, so make sure to talk to the experts in your unit and/or read your ventilator manual before you use them!
Volume Support
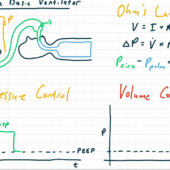
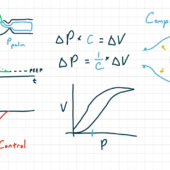
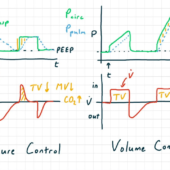
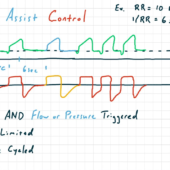
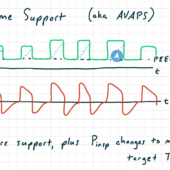
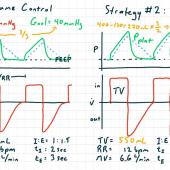
Volume Support mode is a modification to Pressure Support mode. Just like Pressure Support, modes are pressure- or flow-triggered, pressure-limited, and flow-cycled. So the patient controls when the breath starts and stops, and the patient's compliance has a big effect on how much tidal volume is drawn with each breath. The big difference from Pressure Support is that in Volume Support mode, the operator doesn't set the inspiratory directly. Instead, they set the tidal volume. Then, just like in Pressure Regulated Volume Control mode, the ventilator computer monitors the tidal volume achieved with each breath, and adjusts the inspiratory pressure automatically as needed to hit the assigned target.
Proportional Assist Ventilation
Taking the computer control of the inspiratory valve to the next level, Proportional Assist Ventilation changes the ventilator's circuit pressure multiple times per second in order to tailor the ventilator's support to the patient's effort. The resulting circuit pressure is based on physiological models continuously calculated by the ventilator computer.
In Proportional Assist Ventilation, the operator sets the percent of respiratory effort for the ventilator to take on. If the patient takes a big breath, the ventilator provides more inspiratory pressure than if the patient takes a smaller breath. This mode is extremely comfortable for patients, reduces fatigue of the respiratory musculature, and can be weaned well by slowly transferring respiratory effort back to the patient.
Automatic Tube Compensation
Similar to the above, Automatic Tube Compensation is a computationally intensive ventilator mode, which adjusts the circuit pressure multiple times per second. In this mode, the operator programs the details of the endotracheal tube or tracheostomy device into the ventilator, and the ventilator computer then adjusts the circuit pressure to compensate for the added resistance of the tube. Automatic Tube Compensation can be used on its own as a weaning mode, or added to another primary ventilator mode.
Mandatory Minute Ventilation
Mandatory Minute Ventilation is a mode that attempts to balance comfortable oxygenation with consistent ventilation. At its base, Mandatory Minute Ventilation is very similar to Volume Support mode: breaths are pressure- or flow-triggered, pressure-limited, and flow-cycled. However, to address periods of apnea or bradypnea, in Mandatory Minute Ventilation, the ventilator computer monitors the patient's minute ventilation breath-by-breath. If the minute ventilation is falling short, the ventilator triggers additional Volume Control breaths to make up the difference.
This talk concludes our deep dive into conventional ventilator modes. As a concluding thought, consider the three broad levels of "reactiveness" that the various ventilator modes span. The most basic modes, like Pressure and Volume Control and Assist/Control, and Pressure Pupport, do the same thing every breath. Although this doesn't allow the ventilator to react to changing physiology, it has the advantage of being very predictable.
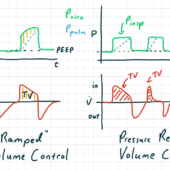
At the next level, "servo" modes like Pressure Regulated Volume Control and Volume Support adjust their limit variables every breath. These modes have the advantage of being able to react to changes in the patient's physiology, but they do so by introducing changes that must be understood and monitored. Finally, "adaptive" modes like Proportional Support Ventilation and Automatic Tube Compensation run calculations and change the circuit pressure multiple times per second. This allows fantastic meshing between the ventilator and patient, but also demands heightened understanding of the operator, as failure modes may not always be obvious.
Now that we've concluded our initial foray into ventilator modes, next we'll dive into the physiology of hypoventilation and hypoxemia, so we can work to treat respiratory failure with a ventilator.
Patient-Triggered Breaths
Comments
This post currently has no responses.