
The Basic Ventilator
 John McManigle | 3 May 2020
John McManigle | 3 May 2020
This is the first video in our Pulmonary and Ventilator Mechanics Chalk Talk Series, where our goals are to learn how a ventilator works, and how to work a ventilator. The strategy in this whole series is to start off with a very simple patient-ventilator system. Then, as the talks progress, we'll add complexity -- in terms of both patient pathology and ventilator capability -- until we are ventilating a challenging ARDS patient on a modern ICU ventilator.
With that strategy in mind, this lecture builds up a basic bellows-driven ventilator, and explores in some detail where our standard pressure control and volume control waveforms come from, with reference to Ohm's law of resistance. We finish off by describing standard ventilator settings we use to program these modes.
Intro to the VPMCTS
The goal of the Ventilator and Pulmonary Mechanics Chalk Talk Series is to learn how a ventilator works, and how to work a ventilator. We'll accomplish this through a series of recorded "chalk talks" that explain the mechanics behind the patient-ventilator system. Today, that system will start off very basic: an otherwise healthy, completely paralyzed patient connected to a bellows-driven ventilator. As the talks go on, both the patient and the ventilator will get more complicated.
This is also a "choose your own adventure" type series. The beginner lectures are appropriate for advanced medical or allied health professions students, or maybe an intern who is starting their first ICU rotation after a long time away. The first ten talks, in particular, start very basic and culminate in a great understanding of the tradeoffs in optimizing oxygenation and ventilation in a patient with relatively normal lung function. Then we'll see more advanced lectures that get into some of the trickier pathophysiology and treatments for serious pulmonary disease, like ARDS. We'll also work our way up to advanced ventilator topics, like airway pressure release ventilation (APRV) and oscillators, and touch on some closely related topics that go beyond "just" the ventilator, like prone positioning and ECMO.
The Basic Ventilator
The Basic Ventilator talk begins with a model patient -- healthy lungs, fully paralyzed -- connected to a bellows with ventilator circuit tubing and an endotracheal tube. The question becomes: how do we drive this bellows down to deliver breathing gas to our patient? The two simplest ways, which correspond with the two most basic ventilation modes, are to drive the bellows down at a constant rate with a leadscrew -- the equivalent of volume control ventilation -- and to build a dome around the bellows and fill it with driving gas at a constant pressure -- the equivalent of pressure control ventilation.
Ohm's Law of Resistance
To dive into the pressure and flow graphs that define pressure control and volume control ventilation, first we need to understand Ohm's law. Ohm's law describes the linear relationship between voltage and current in an electrical circuit, V = I × R. In ventilator mechanics, the relationship isn't completely linear, but it's close enough that we use the approximation most of the time. The pressure difference between the ventilator circuit pressure is equal to the product of the volume flow rate of gas moving into the lungs and the airway resistance.
Pressure Control Ventilation
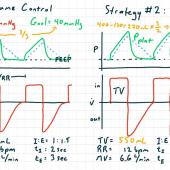
With an understanding of Ohm's Law, we can now explore the pressure-flow relationships in pressure control ventilation. When the bellows and circuit are pressurized at constant pressure P during inspiration, that generates a difference between the circuit pressure and the pulmonary pressure, and a resultant flow of breathing gas into the lungs. As the lungs fill with gas, pulmonary pressure rises, which decreases the pressure difference and decreases the inspiratory flow. When it's time for expiration, the pressure in the circuit drops to our positive end expiratory pressure (PEEP), triggering expiration. Just like inspiration, expiration starts at a relatively high flow and then slows down as the difference between pulmonary and circuit pressures narrows.
Volume Control Ventilation
The analysis of volume control ventilation is very similar to that of pressure control ventilation. The big difference is during inspiration. Because the breath is delivered at constant volume flow rate, the flow graph in volume control is flat during inspiration, while the pressure graph increases to maintain a consistent difference between plateau pressure and pulmonary pressure while inspiration continues. When it's time to cycle to expiration, the expiratory valve opens, just like in pressure control mode, and the circuit pressure returns to PEEP. This triggers an expiratory flow pattern that looks identical to the one in pressure control ventilation.
Ventilator Settings
To wrap up this lecture, we look at the ventilator settings needed to program the pressure control and volume control modes.
In both modes, we need to define the timing of the breaths by setting a respiratory rate. Then we need to divide the respiratory cycle into inspiratory and expiratory phases, either by setting the inspiratory time directly, or by setting the I:E ratio. These choices are equivalent, but will behave differently when you go to change the respiratory rate later.
In pressure control mode, you need to define the inspiratory pressure to set behavior during inspiration. Based on how that inspiratory pressure interacts with your patient's pulmonary mechanics, you'll get your inspiratory flow.
In volume control mode, you program a tidal volume. Based on the tidal volume and inspiratory time settings, the ventilator calculates the required inspiratory flow rate. And based on how that flow rate interacts with your patient's pulmonary mechanics, you'll wind up with your circuit pressure behavior.
Finally, in both modes, you need to define the positive end expiratory pressure, which describes the ventilator's behavior during expiration.
Thanks so much for your attention! Next time, we'll dive a little further into these pressure- and flow-over-time graphs to better understand compliance and resistance, peak and plateau pressures, and our first complication of mechanical ventilation, auto-PEEP.
Comments
This post currently has no responses.